Stroke Is A Major Killer
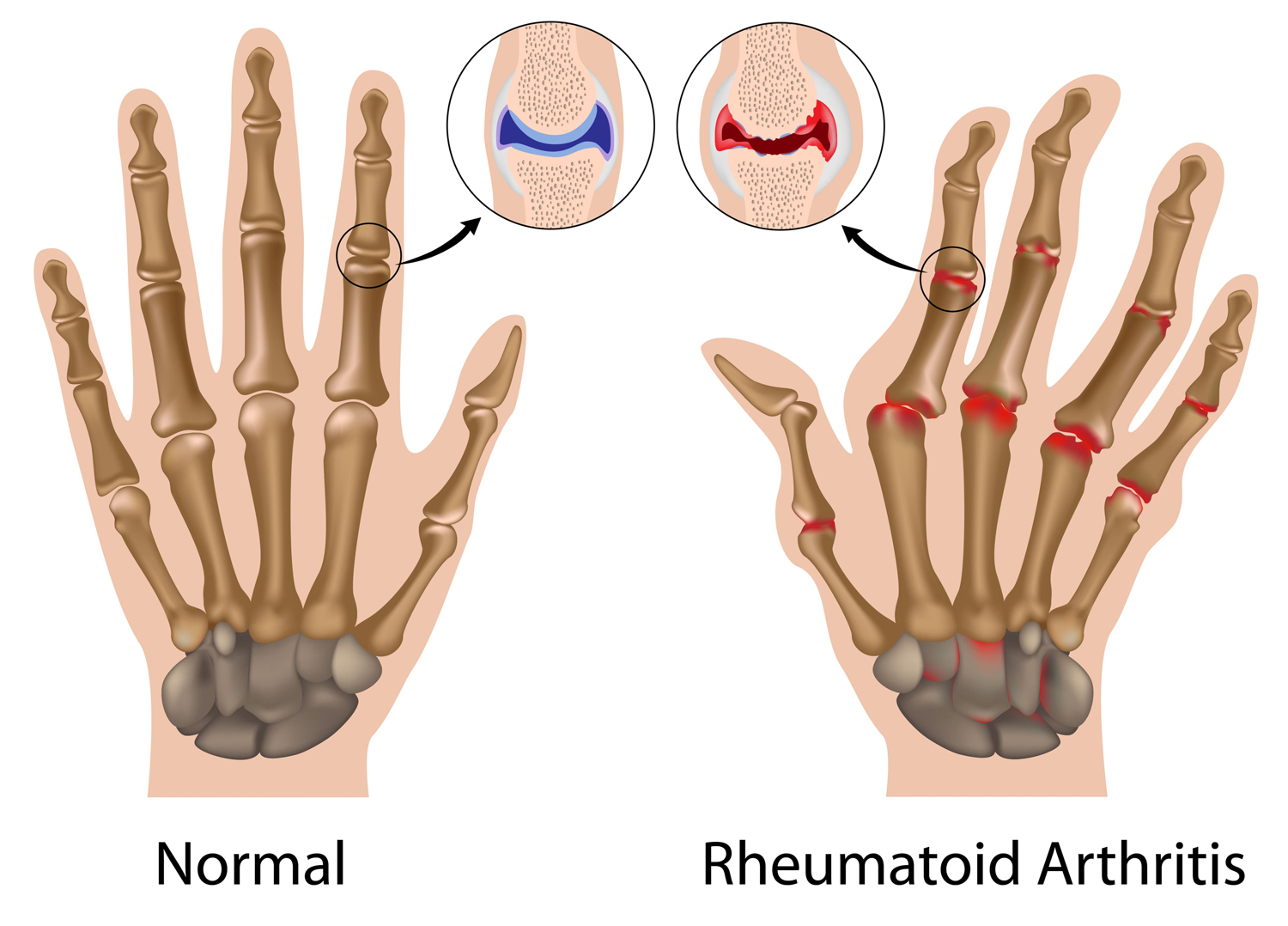
Rheumatoid Arthritis

Rheumatoid arthritis. Increase the risk of heart disease
Rheumatoid arthritis is a chronic disease and recent research indicates that it may increase the risk of heart attacks, strokes, and other heart disease-related problems.
Studies have shown that patients with rheumatoid arthritis are more than twice as likely to suffer from heart disease-related problems, about the same level compared to Type 2 diabetes mellitus. However, this study did not prove any causal relationship. The test was designed to show that rheumatoid arthritis is related to heart disease only.
Joint pain, stiffness, and swelling are the main features of rheumatoid arthritis, but this disease can also cause inflammation of the body’s organs.
Research indicates that systemic chronic inflammation of rheumatoid arthritis is an independent risk factor of heart attack.
Experts opined that, the effective treatments of systemic inflammatory reactions can reduce the risk of heart problems among these patients.
Rheumatoid arthritis :
Surgery or Drug Therapy ?
Case study:
John is a white-collar worker. He discovered a year ago, the joints of his fingers began to stiffen. But as soon as he moved a little, the symptoms disappeared. At first, he didn’t pay much attention to this symptom.
Recently, John felt that something was amiss. He sensed some pains in his fingers’ joints when he woke up in the morning. Eventually, his doctor confirmed he has suffered from rheumatoid arthritis.
The treatment of rheumatoid arthritis can be divided into two categories: non-surgical treatment and surgical treatment. Treatment methods and choices of drugs are depending on the patient’s current health conditions.

In non-surgical treatment, the attending physician will first select non-steroidal anti-inflammatory drugs (NSAIDs) for the patient to reduce and control synovitis within the joint, while reducing the inflamed synovial membrane and slowing down the erosions of cartilage layer and bone ends inside the joint. In terms of improvement of clinical symptoms, patients will feel the reduction of joint swelling, heat and pain. Joint activities will also have a significant improvement after treatments. However, it must be noted that each patient responds differently to various types of nonsteroidal anti-inflammatory drugs.
These drugs may cause side effects such as stomach pain, stomach ulcers and kidney damage. However, some new generations drugs have managed to reduce the damages of stomach and kidneys.
There are certain degree of risks and benefits in drug therapy, so it is imperative that patients follow doctors’ instructions rather than completely shutting out drug treatment. Drug therapy also includes topical anti-inflammatory drugs, tapes, and gels. The roles are allowing drugs to penetrate directly into joint tissues to reduce and control inflamed lesions.

Drug selection
Controlling acute inflammation
To some patients, non-steroidal anti-inflammatory drugs alone cannot control and treat the inflammation of joints. It is necessary to use disease-modifying anti-rheumatic drugs known as “disease-responsive drug therapy” (DMARDs). These drugs include drugs such as Penicillamine, Gold, Chloroquine, and Methotrexate. Often many patients need to use the first group of non-steroidal anti-inflammatory drugs, together with the second group of DMARDs, to achieve the goal of controlling the disease.
Steroids are the third group of drugs whose main function is to control the synovitis within the joints. By using steroids and the other two groups of drugs simultaneously, it will give effective control on synovial inflammation. Long-term use of high levels of steroids may lead to hormonal disorders and severe osteoporosis.

The attending doctor may also equip the patient with “immunological modulation” treatment, to adjust and strengthen the patient’s immune system for controlling patient’s rheumatoid arthritis. After all, this type of arthritis is a problem that related to patient’s immune system.
Affected joints such as fingers, knees, ankles, etc., may also require injection of steroids at the joints so that steroids can directly reduce the inflammation of the synovial membrane within the joints. With oral and topical medications, patients with acute inflammation of the joints will be more quickly controlled.
The joints affected by rheumatoid arthritis present with clinical symptoms of swelling, fever, and pain. In addition to drug treatments to reduce joint inflammation, the rehabilitation therapist will equip the patient with a stent that protects the joints and tendons, reducing joint and tendon activity and thus reducing pains. At the same time, perform some low-impact but strong muscle movements around the joints to help protect the affected joints and help reduce and ease the destruction of the joints.

Surgical treatment
As for surgical treatment, some patients suffer from severe and long-term and repetitive inflammation of the joint membrane, the cartilage layer inside the joint is severely corroded, and the joints are also deformed. The movements of patients are severely restricted, and their quality of lives is also greatly affected. Surgical treatment is the last resort.
Arthroscopic resection is the removal of the inflamed synovium inside the joint to reduce the damage of the synovial membrane to the joint.
Surgery can be performed with an open resection of the synovial membrane or an endoscopic surgical procedure. In general, drug treatments can control and treat synovial inflammation, but some patients’ synovitis cannot be controlled by drugs, thus surgical resection plays a very important role under such circumstance.
For replacement surgery, the most common joints are the hip and knee joints. However, for patients suffering from “rheumatoid arthritis,” other joints such as shoulder joints, elbow joints, wrist joints and palms, and even finger joints can undergo joint replacement surgery.
Patients undergoing joint replacement surgery, coupled with appropriate rehabilitation therapy, can generally be effective within short period of time and patients’ quality of lives can be greatly improved.
In sports, when the patient is acutely inflamed, the patient should not perform excessive joint exercise. Especially pressured joints, such as knee joints and ankle joints. Once acute inflammation is controlled, strong muscle ligament movement or movement of the active joints, are also suitable for many patients despite the presence of rheumatoid arthritis.
Note : This article is meant for reference of public only. Should you have any question after reading it, please consult medical professional.
Source : Original article is printed by Sin Chew Daily, Malaysia.
Related posts





